Is the Increasing Incidence of Thyroid Cancer in the Nordic Countries Caused by Use of Mobile Phones?


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Methods
3. Results
3.1. The Swedish Cancer Register
3.2. NORDCAN
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schneider, A.B. Radiation-induced thyroid tumors. Endocrinol. Metab. Clin. N. Am. 1990, 19, 495–508. [Google Scholar] [CrossRef]
- Quimby, E.H.; Werner, S.C. Late Radiation Effects in Roentgen Therapy for Hyperthyroidism. JAMA 1949, 140, 1046–1047. [Google Scholar] [CrossRef]
- Duffy, B.J.; Fitzgerald, P.J. Thyroid cancer in childhood and adolescence; a report on 28 cases. Cancer 1950, 3, 1018–1032. [Google Scholar] [CrossRef]
- Hallquist, A.; Hardell, L.; Löfroth, P.O. External radiotherapy prior to thyroid cancer: A case-control study. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 1085–1089. [Google Scholar] [CrossRef]
- Prentice, R.L.; Kato, H.; Yoshimoto, K.; Mason, M. Radiation exposure and thyroid cancer incidence among Hiroshima and Nagasaki residents. Natl. Cancer Inst. Monogr. 1982, 62, 207–212. [Google Scholar]
- Tsuda, T.; Tokinobu, A.; Yamamoto, E.; Suzuki, E. Thyroid Cancer Detection by Ultrasound Among Residents Ages 18 Years and Younger in Fukushima, Japan: 2011 to 2014. Epidemiology 2016, 27, 316–322. [Google Scholar] [CrossRef] [Green Version]
- Zablotska, L.; Nadyrov, E.; Rozhko, A.; Gong, Z.; Polyanskaya, O.; McConnell, R.; O’Kane, P.; Brenner, A.; Little, M.P.; Ostroumova, E.; et al. Analysis of thyroid malignant pathological findings identified during three rounds of screening (1997–2008) of a Belarusian cohort of children and adolescents exposed to radioiodines after the Chernobyl accident. Cancer 2015, 121, 457–466. [Google Scholar] [CrossRef] [Green Version]
- Tondel, M.; Hjalmarsson, P.; Hardell, L.; Carlsson, G.; Axelson, O. Increase of regional total cancer incidence in north Sweden due to the Chernobyl accident? J. Epidemiol. Community Health 2004, 58, 1011–1016. [Google Scholar] [CrossRef] [Green Version]
- Hallquist, A.; Hardell, L.; Degerman, A.; Boquist, L. Thyroid cancer: Reproductive factors, previous diseases, drug intake, family history and diet. A case-control study. Eur. J. Cancer Prev. 1994, 3, 481–488. [Google Scholar] [CrossRef]
- Cao, Y.; Wang, Z.; Gu, J.; Hu, F.; Qi, Y.; Yin, Q.; Sun, Q.; Li, G.; Quan, B. Reproductive Factors but Not Hormonal Factors Associated with Thyroid Cancer Risk: A Systematic Review and Meta-Analysis. Biomed Res. Int. 2015, 2015, 103515. [Google Scholar] [CrossRef] [Green Version]
- Carlberg, M.; Hedendahl, L.; Ahonen, M.; Koppel, T.; Hardell, L. Increasing incidence of thyroid cancer in the Nordic countries with main focus on Swedish data. BMC Cancer 2016, 16, 426. [Google Scholar] [CrossRef] [Green Version]
- Vigneri, R.; Malandrino, P.; Vigneri, P. The changing epidemiology of thyroid cancer: Why is incidence increasing? Curr. Opin. Oncol. 2015, 27, 1–7. [Google Scholar] [CrossRef]
- Adas, M.; Adas, G.; Koc, B.; Ozulker, F. Incidental thyroid lesions on FDG-PET/CT: A prevalence study and proposition of management. Minerva Endocrinol. 2015, 40, 169–175. [Google Scholar]
- Lauer, O.; Frei, P.; Gosselin, M.-C.; Joseph, W.; Röösli, M.; Fröhlich, J. Combining near- and far-field exposure for an organ-specific and whole-body RF-EMF proxy for epidemiological research: A reference case. Bioelectromagnetics 2013, 34, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Luo, J.; Deziel, N.C.; Huang, H.; Chen, Y.; Ni, X.; Ma, S.; Udelsman, R.; Zhang, Y. Cell phone use and risk of thyroid cancer: A population-based case-control study in Connecticut. Ann. Epidemiol. 2019, 29, 39–45. [Google Scholar] [CrossRef]
- Luo, J.; Li, H.; Deziel, N.C.; Huang, H.; Zhao, N.; Ma, S.; Ni, X.; Udelsman, R.; Zhang, Y. Genetic susceptibility may modify the association between cell phone use and thyroid cancer: A population-based case-control study in Connecticut. Environ. Res. 2020, 182, 109013. [Google Scholar] [CrossRef]
- National Toxicology Program. NTP Technical Report on the Toxicology and Carcinogenesis Studies in B6C3F1/N Mice Exposed to Whole-Body Radio Frequency Radiation at a Frequency (1900 MHz) and Modulations (GSM and CDMA) Used by Cell Phones. 2018. Available online: https://ntp.niehs.nih.gov/ntp/about_ntp/trpanel/2018/march/tr596peerdraft.pdf (accessed on 27 October 2020).
- National Toxicology Program. NTP Technical Report on the Toxicology and Carcinogenesis Studies in Hsd:Sprague Dawley sd Rats Exposed to Whole-Body Radio Frequency Radiation at a Frequency (900 MHz) and Modulations (GSM and CDMA) Used by Cell Phones. Available online: https://ntp.niehs.nih.gov/ntp/about_ntp/trpanel/2018/march/tr595peerdraft.pdf (accessed on 27 October 2020).
- Hardell, L.; Carlberg, M. Comments on the US National Toxicology Program technical reports on toxicology and carcinogenesis study in rats exposed to whole-body radiofrequency radiation at 900 MHz and in mice exposed to whole-body radiofrequency radiation at 1900 MHz. Int. J. Oncol. 2019, 54, 111–127. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Caumo, S.; Vicente, A.; Custódio, D.; Alves, C.; Vasconcellos, P. Organic compounds in particulate and gaseous phase collected in the neighbourhood of an industrial complex in São Paulo (Brazil). Air Qual. Atmos. Health 2018, 11, 271–283. [Google Scholar] [CrossRef]
- Shore, R.E.; Hempelmann, L.H.; Woodward, A.D. Carcinogenic effects of radiation on the human thyroid gland. In Radiation Carcinogenesis; Upton, A.C., Albert, R.E., Burns, F.J., Shore, R.E., Eds.; Elsevier: New York, NY, USA, 1986; pp. 293–309. [Google Scholar]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef] [Green Version]
- Sanabria, A.; Kowalski, L.P.; Shah, J.P.; Nixon, I.J.; Angelos, P.; Williams, M.D.; Rinaldo, A.; Ferlito, A. Growing incidence of thyroid carcinoma in recent years: Factors underlying overdiagnosis. Head Neck 2018, 40, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Vaccarella, S.; Dal Maso, L.; Laversanne, M.; Bray, F.; Plummer, M.; Franceschi, S. The Impact of Diagnostic Changes on the Rise in Thyroid Cancer Incidence: A Population-Based Study in Selected High-Resource Countries. Thyroid 2015, 25, 1127–1136. [Google Scholar] [CrossRef] [PubMed]
- Socialstyrelsen [The National Board of Health and Welfare]. Statistics on Cancer Incidence 2018. Available online: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2019-12-6525.pdf (accessed on 5 December 2020).
- Wingren, G.; Hallquist, A.; Hardell, L. Diagnostic X-ray exposure and female papillary thyroid cancer: A pooled analysis of two Swedish studies. Eur. J. Cancer Prev. 1997, 6, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Braganza, M.Z.; Potischman, N.; Park, Y.; Thompson, F.E.; Hollenbeck, A.R.; Kitahara, C.M. Adolescent and mid-life diet and subsequent risk of thyroid cancer in the NIH-AARP Diet and Health Study. Int. J. Cancer 2015, 137, 2413–2423. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
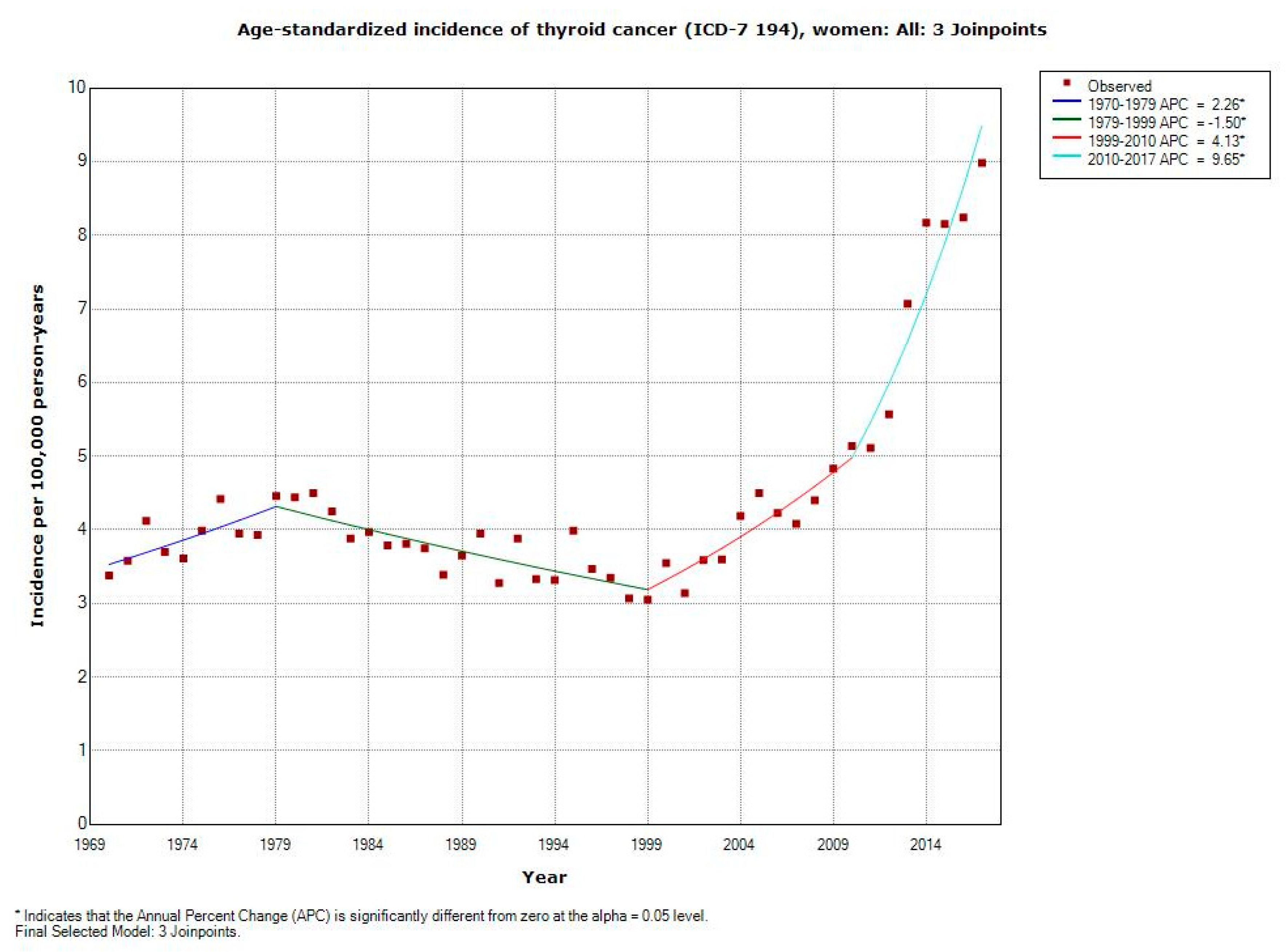
| ICD-7 | Joinpoint Location | APC 1 (95% CI) | APC 2 (95% CI) | APC 3 (95% CI) | APC 4 (95% CI) | AAPC (95% CI) |
|---|---|---|---|---|---|---|
| 194 | ||||||
| All women (n = 13,020) | 1979; 1999; 2010 | +2.26 (+0.36, +4.20) | −1.50 (−2.10, −0.90) | +4.13 (+2.48, +5.81) | +9.65 (+6.68, +12.71) | +2.13 (+1.43, +2.83) |
| 0–19 years (n = 318) | No joinpoint detected | - | - | - | - | +1.69 (+0.88, +2.51) |
| 20–39 years (n = 2935) | 2002 | +0.53 (+0.07, +0.99) | +7.16 (+5.64, +8.70) | - | - | +2.60 (+2.05, +3.15) |
| 40–59 years (n = 4223) | 2002 | −0.95 (−1.60, −0.29) | +7.39 (+5.20, +9.63) | -- | - | +1.64 (+0.85, +2.43) |
| 60–79 years (n = 4166) | 1974; 2003 | +9.50 (−2.44, +22.91) | −2.11 (−2.70, −1.52) | +6.00 (+4.20, +7.83) | - | +1.20 (+0.06, +2.35) |
| 80+ years (n = 1378) | 1979; 1996 | +2.40 (−1.75, +6.73) | −4.57 (−6.22, −2.90) | +0.52 (−0.63, +1.69) | - | −1.00 (−2.08, +0.10) |
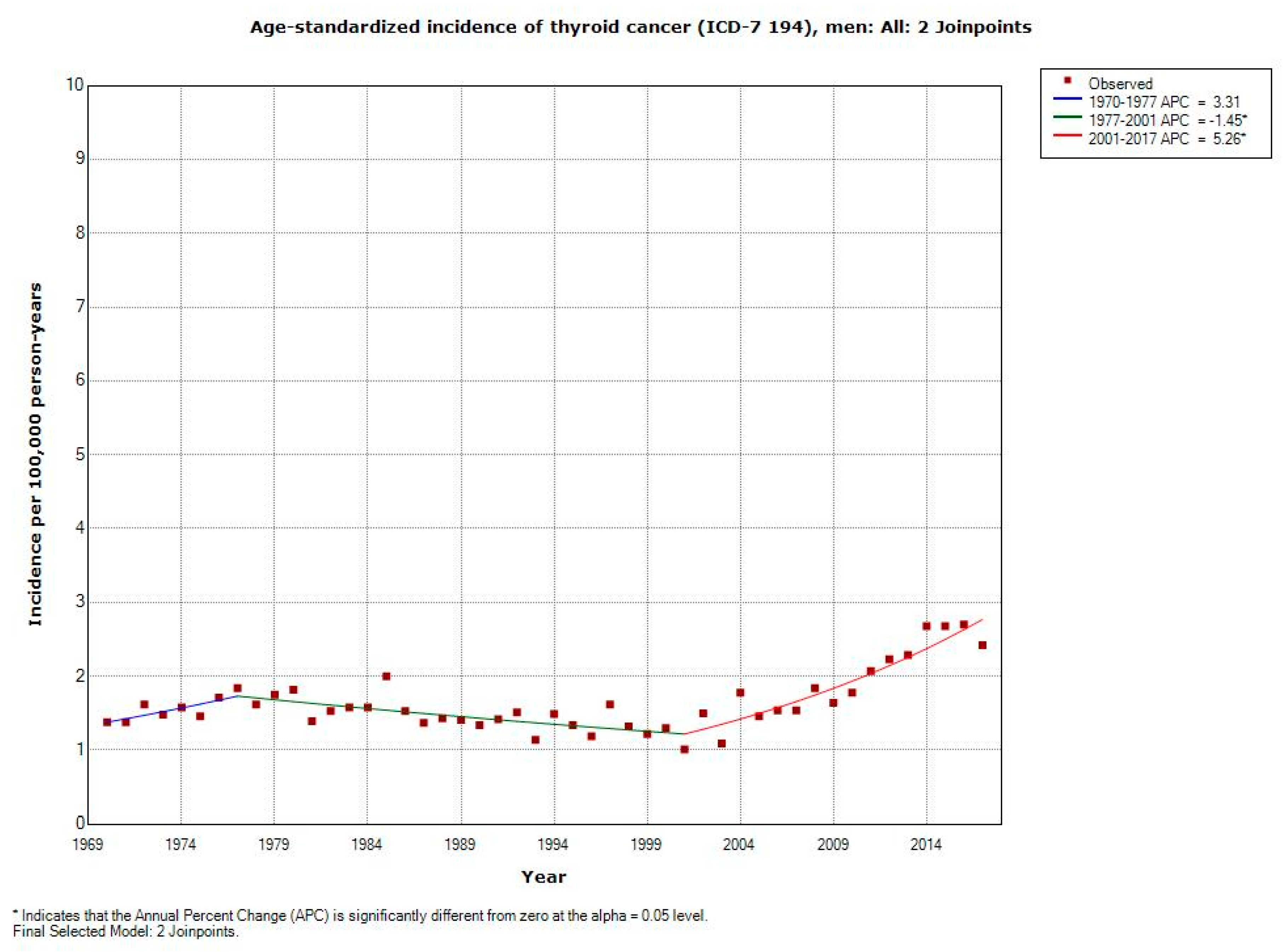
| ICD-7 | Joinpoint Location | APC 1 (95% CI) | APC 2 (95% CI) | APC 3 (95% CI) | AAPC (95% CI) |
|---|---|---|---|---|---|
| 194 | |||||
| All men (n = 5047) | 1977; 2001 | +3.31 (−0.78, +7.56) | −1.45 (−2.11, −0.79) | +5.26 (+4.05, +6.49) | +1.49 (+0.71, +2.28) |
| 0–19 years (n = 98) | - | - | - | - | - |
| 20–39 years (n = 800) | 2001 | −0.67 (−1.92, +0.60) | +7.80 (+4.17, +11.54) | - | +2.13 (+0.72, +3.57) |
| 40–59 years (n = 1508) | 2003 | −0.58 (-1.25, +0.09) | +5.54 (+2.99, +8.16) | - | +1.21 (+0.36, +2.06) |
| 60–79 years (n = 2184) | 1980; 2001 | +2.69 (−0.10, +5.56) | −2.52 (−3.46, −1.57) | +4.77 (+3.36, +6.20) | +1.02 (+0.17, +1.87) |
| 80+ years (n = 457) | No joinpoint detected | - | - | - | −1.45 (−2.64, −0.24) |
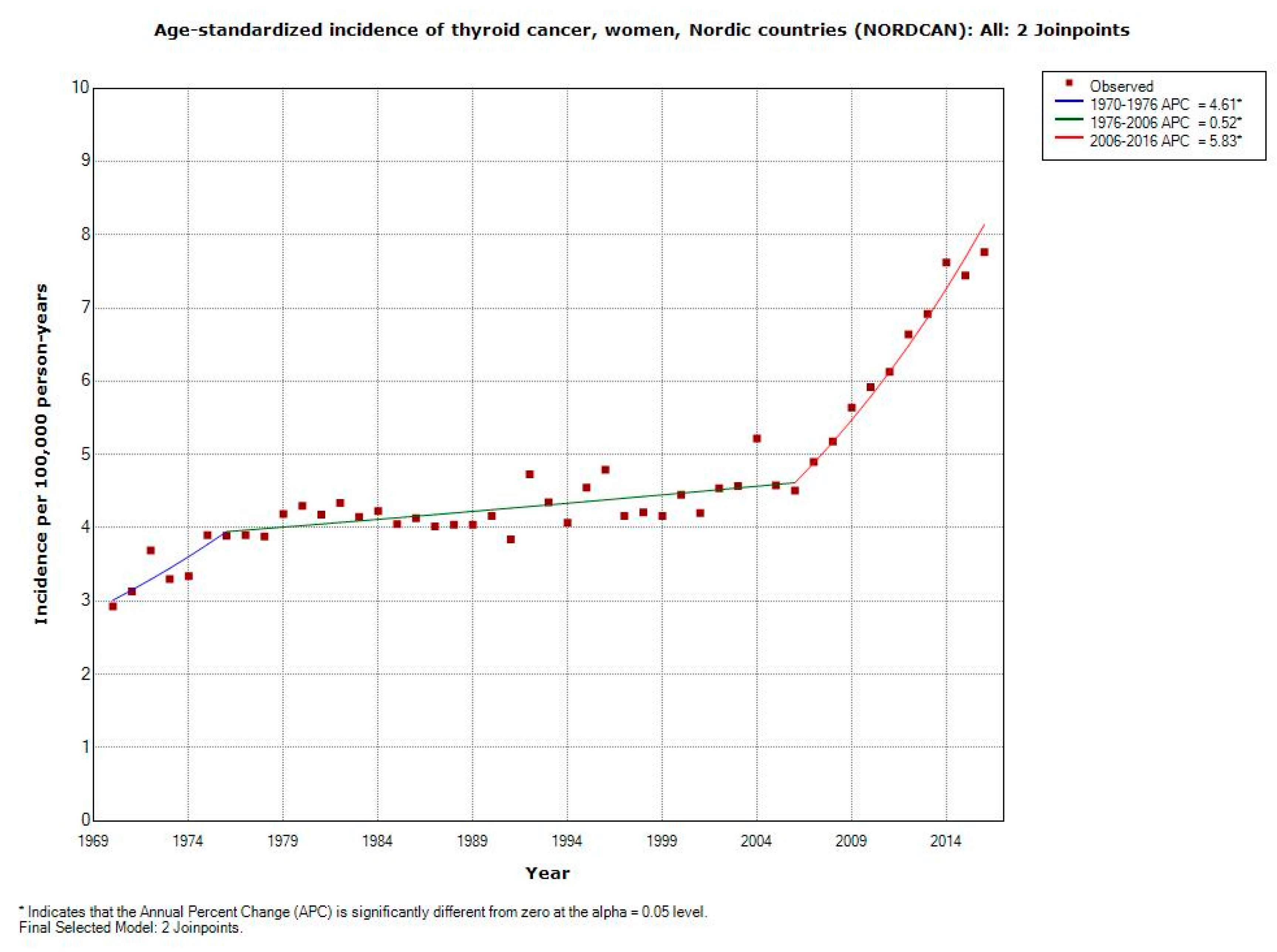
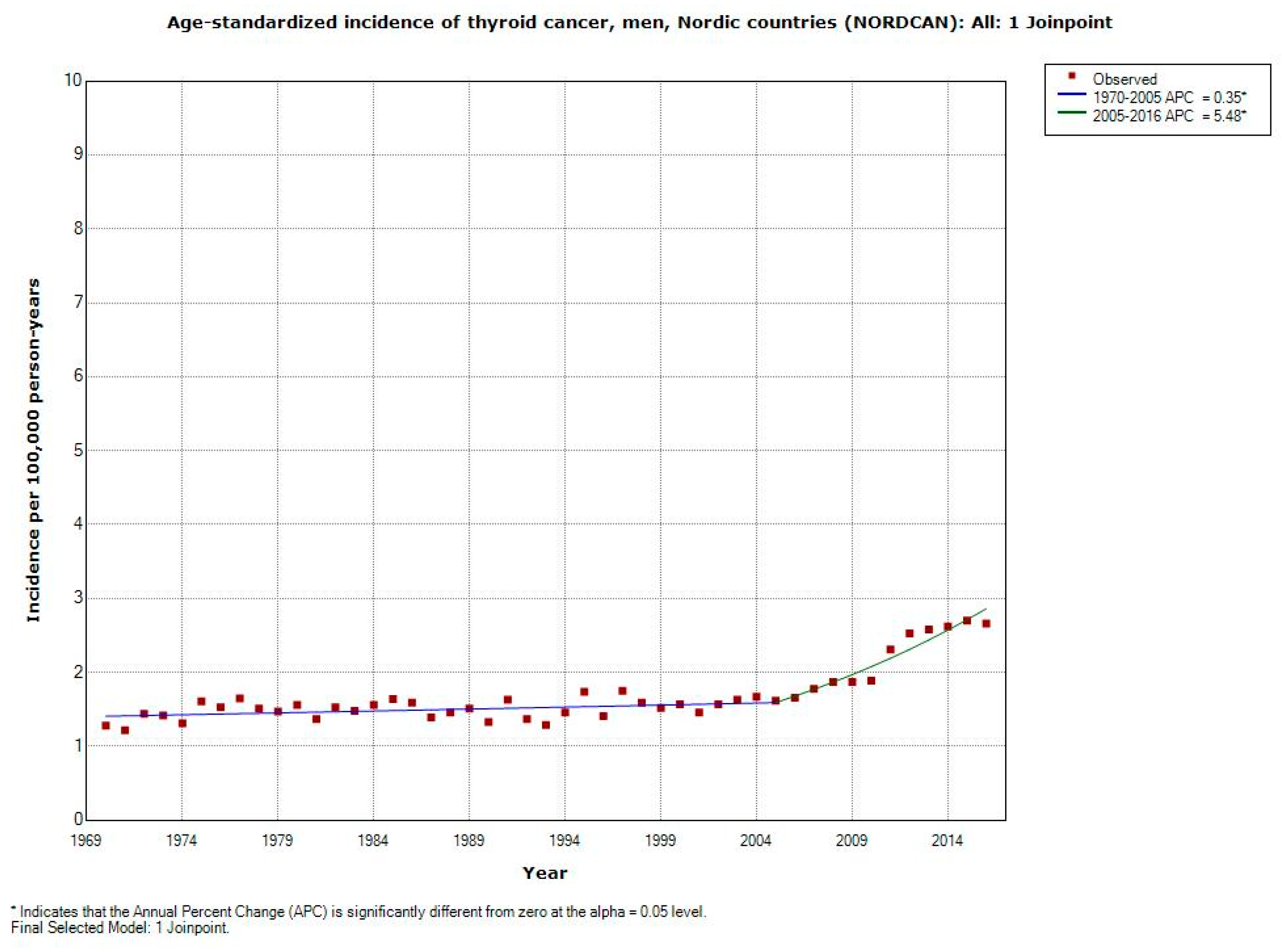
| ICD-10 | Joinpoint Location | APC 1 (95% CI) | APC 2 (95% CI) | APC 3 (95% CI) | AAPC (95% CI) |
|---|---|---|---|---|---|
| C73 | |||||
| All women (n = 36,050) | 1976; 2006 | +4.61 (+1.90, +7.39) | +0.52 (+0.28, +0.77) | +5.83 (+4.56, +7.12) | +2.18 (+1.73, +2.64) |
| All men (n = 13,078) | 2005 | +0.35 (+0.09, +0.61) | +5.48 (+3.92, +7.06) | - | +1.55 (+1.15, +1.96) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carlberg, M.; Koppel, T.; Hedendahl, L.K.; Hardell, L. Is the Increasing Incidence of Thyroid Cancer in the Nordic Countries Caused by Use of Mobile Phones? Int. J. Environ. Res. Public Health 2020, 17, 9129. https://doi.org/10.3390/ijerph17239129
Carlberg M, Koppel T, Hedendahl LK, Hardell L. Is the Increasing Incidence of Thyroid Cancer in the Nordic Countries Caused by Use of Mobile Phones? International Journal of Environmental Research and Public Health. 2020; 17(23):9129. https://doi.org/10.3390/ijerph17239129
Chicago/Turabian StyleCarlberg, Michael, Tarmo Koppel, Lena K. Hedendahl, and Lennart Hardell. 2020. "Is the Increasing Incidence of Thyroid Cancer in the Nordic Countries Caused by Use of Mobile Phones?" International Journal of Environmental Research and Public Health 17, no. 23: 9129. https://doi.org/10.3390/ijerph17239129