
Abstract
Attention deficit hyperactivity disorder (ADHD) is a common neuropsychiatric condition often persisting into adulthood, characterized by inattention, impulsivity, and hyperactivity. Emerging research suggests a connection between ADHD and gut microbiota, highlighting probiotics as potential therapeutic agents. This study involved a double-blind, randomized controlled trial where college students with ADHD received either a multi-strain probiotic supplement or a placebo daily for three months. ADHD symptoms were evaluated using a computerized performance test (MOXO) and the MATAL questionnaire. Academic records provided performance data. Additionally, eating and sleeping habits, gastrointestinal symptoms, and anthropometrics were assessed through questionnaires before and after the intervention. Fingernail cortisol concentrations (FCC) measured the long-term activity of the hypothalamic–pituitary–adrenal axis. The findings indicated that the probiotic significantly decreased hyperactivity, improved gastrointestinal symptoms, and enhanced academic performance. A multivariate analysis identified age as a significant predictor, with younger participants experiencing greater overall benefits from the intervention. There was also a negative correlation between FCC and symptoms of attention and impulsivity. Furthermore, higher academic grades were associated with lower levels of hyperactivity and impulsivity. These results suggest a beneficial impact of probiotics on ADHD symptoms and lay the groundwork for further studies to evaluate the effects of various probiotic strains on clinical outcomes in ADHD.
Similar content being viewed by others
Introduction
Attention deficit hyperactivity disorder (ADHD) is a neurodevelopmental disorder characterized by persistent patterns of inattention, hyperactivity, and impulsivity that interfere with functioning or development1. In adults, ADHD affects 3–4% of the population2,3, with symptoms that can include difficulties in maintaining employment, challenges in forming and sustaining relationships with family members, friends, partners, or co-workers, problems with substance use, and trouble coping with stress4. Although ADHD can also impact academic performance, particularly among college students5, the broader implications for work and social functioning are more representative of the adult experience. While ADHD can cause significant impairment in both children and adults, the manifestations observed in adults with ADHD may appear more severe and impairing due to the persistence of symptoms combined with the development of comorbidities, such as anxiety, mood disorders, and substance use disorders, which often exacerbate the condition4,6.
In recent years, the etiological and developmental frameworks of ADHD have undergone significant reconceptualization, increasingly highlighting the dysregulation of arousal systems as a foundational aspect of the disorder7. Modern theoretical models propose that ADHD involves a complex interplay between emotional dysregulation and neurocognitive discrepancies, thereby implicating the autonomic nervous system (ANS) and the hypothalamic-pituitary-adrenal (HPA) axis within its etiological domain8. This perspective emphasizes the critical interdependence of stress responsiveness and emotion regulation processes, suggesting that abnormal diurnal cortisol secretion patterns and cortisol hyperreactivity, hallmarks of HPA axis dysregulation, are correlated with ADHD’s behavioral manifestations, notably impulsivity9. Despite empirical evidence indicating altered cortisol rhythms in individuals diagnosed with ADHD10, the understanding of these physiological processes remains elusive. A recent meta-analytic review highlighted the complexity of this relationship, finding no significant association between ADHD diagnosis in childhood and variations in cortisol reactivity under controlled stress conditions11.
Recent studies show that under stress situations, probiotics, may play a beneficial role by regulating the synthesis and release of a variety of neurotransmitters and bioactive factors including cortisol12, and to some extent improve the stress-related physical and psychiatric symptoms in adults13,14. These effects we shown to involve the microbiota–gut–brain axis (MGBA), defined as the bidirectional relationship between the gut microbiota and the central nervous system (CNS) through neural, hormonal, and immunological pathways15. An altered MGBA contributes to the presence of the core symptoms of ADHD as well as the comorbidities, such as sleep disorders16.
Given the links between gut microbiota and ADHD mechanisms, modulation of gut bacteria composition with probiotic supplements is a promising treatment strategy. Psychobiotics, a group of probiotics, have been shown in vitro to produce and serve as a delivery mechanism for neuroactive substances such as gamma-aminobutyric acid (GABA) and serotonin, affecting the MGBA17. Additionally, in vivo studies have shown their ability to improve gastrointestinal (GI) function, mood, cognition, and anxiety (14). Lactobacillus (L) and Bifidobacterium (B), typical bacterial inhabitants of the human gut, have been extensively studied for their probiotic and psychobiotic effects (15). Some of the bacteria from these and other genera, such as B. helveticus, B. longum, B. animalis, Bacillus subtilis and Enterococcus faecium, have been reported to produce or promote the synthesis of neurotransmitters in the gut18,19,20,21,22,23,24, consequently modulating MGBA pathways and affecting behavior25,26,27,28,29.
Furthermore, probiotic supplementation showed positive effects on ADHD symptoms among children, though much of the evidence comes from open trials rather than randomized controlled trials (RCTs)21. For example, Pärtty and colleagues conducted a long-term study where L. rhamnosus GC supplementation in at-risk infants (3 months old) reduced the incidence of ADHD diagnosis when followed up for 13 years30. In another open-label trial, 30 children diagnosed with ADHD showed improved inattention and hyperactive/impulsive symptoms while receiving B. bifidum (Bf-688) for 8 weeks31. Additionally, L. helveticus and B. longum strains were reported to inhibit inflammation and decrease cortisol levels, resulting in an amelioration of the symptoms of anxiety and depression32. While these results support the potential clinical benefits of probiotic supplementation in children with ADHD, recent studies, such as Wang et al.33, have highlighted the importance of distinguishing between findings in pediatric ADHD populations and those in adults. Wang et al. employed Mendelian Randomization to explore causal relationships between unsaturated fatty acids and ADHD, concluding that there was no significant causal link in adults. This underscores the need for caution when extrapolating results from children to adult ADHD populations. While preliminary open-label trials suggest that probiotics may offer some benefit to children with ADHD, these findings are not yet supported by robust randomized controlled trials, and thus the effects in both children and adults remain uncertain and require further investigation.
We conducted a three-month, clinical trial in college students with ADHD testing the effect of a probiotic mix containing L. helveticus, B. animalis ssp. lactis, Enterococcus faecium, B. longum and Bacillus subtilis on ADHD symptoms, academic achievements, fingernail cortisol concentrations (FCC), GI symptoms and sleep quality. As Lactobacillus and Bifidobacterium strains, alone and in combination show clinical benefits to ADHD children, we hypothesized that the suggested probiotic mix would result in positive clinical effects to ADHD college students and constitute an alternative for the treatment of their symptoms.
Materials and methods
This study was approved by the Ziv Medical Center ethics committee (approval no 0040-16-ZIV) and registered at https://clinicaltrials.gov (registration no NCT02908802) and all experiments were performed in accordance with their relevant guidelines and regulations. All participants signed an informed consent form, and all study procedures were consistent with Good Clinical Practice.
Study design
Participant recruitment
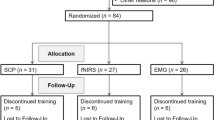
Sixty-seven students from the Tel Hai Academic College Support Center were recruited by institutional emails. We determined the sample size using the WinPepi software34 applying a randomized clinical trial sample size formula considering type I (α) and type II errors (β) of 0.05 and 0.20 (power = 80%), respectively. Based on a previous study35, we used a standard deviation of 6.4 and 4.8 (intervention and placebo, respectively) and a difference in mean of 4.2, considering the decrease in the Beck Depression Inventory score as the key variable. The sample size resulted in 67 when a 15% dropout was added. Eligibility criteria for participation were enrolled students, aged 19–30 years, with an ADHD diagnosis performed by a computerized didactic assessment (MATAL), confirmed by a psychiatrist or neurologist, and not on ADHD medication. Exclusion criteria were antibiotic or probiotic supplementation, dairy intolerance, soy allergy, pregnancy, and serious illnesses (e.g., cancer, HIV/AIDS). Eligible students who provided informed consent were randomly assigned (1:1) to receive either a probiotic or placebo treatment (34 in the intervention arm and 33 in the control arm). The randomization scheme was computerized and was unknown to the participants, researchers, outcome assessors and data analysts until all analyses were completed.
Study intervention
Participants were instructed to consume two capsules (probiotic or placebo) once a day, for three months. The probiotic supplement contained 8 × 109 colony-forming units (CFU) of each of the strains L. helveticus, B. animalis ssp. lactis, Enterococcus faecium, B. longum and Bacillus subtilis. The placebo supplement consisted of potato starch, magnesium stearate and ascorbic acid. Both the probiotic and placebo capsules were generously donated by the Altman Health Company and stored at room temperature at the Tel-Hai College Support Center. The company was not involved in the study design, data collection, analysis of data, manuscript drafting, or submission.
To enhance compliance, participants received daily reminders via WhatsApp messages, scheduled according to their preference, either in the morning or evening. Additionally, participants were required to return the empty supplement packages each month before receiving a new supply. Students who failed to consume at least 80% of the required capsules were withdrawn from the study.
Participants filled in dietary and quality-of-life questionnaires, their height and weight were registered, and fingernail samples were collected at baseline (before starting the intervention-T0) and after 3 months of intervention (T1). To ensure the accuracy and completeness of collected data, all questionnaires and measurements in this study were performed at the Tel Hai Support Center, specifically designed to accommodate students with ADHD, and under the supervision of one of the study’s researchers.
Measurements
Anthropometrics and academic achievement
Anthropometric measurements were taken once a month during the study period. Fat percentage and waist circumference were measured using a bioelectrical impedance analysis (BIA) device and a tape measure, respectively. Height was measured at baseline using a calibrated scale. Body mass index (BMI) was calculated with the formula = (weight/(height)2), at the beginning and end of the study.
To assess the impact of probiotic consumption on academic performance, average grades of the courses the student was enrolled in at the outset (semester before the intervention) and conclusion of the study (semester during treatment) were collected from participant score records.
Dietary habits
Dietary profiling was performed using the validated 127-item FFQ developed for the Israeli population36. Briefly, participants report on their ingestion habits over the preceding year, of 127 food items, with nine frequency options ranging from “never or less than once monthly” to “six or more times daily.” The questionnaire is semi-quantitative, describing each food item’s standard portion size, determined based on information from the Israeli Ministry of Health. The questionnaire was self-administered electronically with the aid of an interviewer. Completeness of the data was ensured by a pop-up notice that appeared when a question was not answered. All participants had a monthly session with a dietitian and were asked to fill out a 24-recall questionnaire37. The participants received no nutritional intervention or dietary guidelines during the study.
Quality-of-life
Participants completed the Family Eating and Activity Habits Questionnaire (FEAQ)38, the School Sleep Habits Survey (SSHS) questionnaire39 and a self-assessment GI symptoms questionnaire40 before and after the three-month intervention. The FEAQ comprises 36 questions categorized into four sections: activity level, exposure to eating-promoting cues, responsiveness to hunger and fullness signals and eating style. The SSHS questionnaire contains eight questions and is administered to assess various aspects of sleep patterns, including daytime and nighttime sleep patterns during both the week and weekends, as well as factors such as sleep duration, bedtime and wake-up time. The GI symptoms questionnaire consists of 21 items categorized into esophageal symptoms, upper gastrointestinal motility issues, bowel symptoms, diarrhea and constipation. Participants reported the frequency of these symptoms, ranging from “never” to “many times during the day”.
ADHD symptoms and severity
All participants underwent the MOXO computerized performance test (MOXO-CPT) at the study baseline and again after three months of intervention. The MOXO-CPT assesses attention, hyperactivity, impulsivity, and timing. In this test, lower scores indicate better performance, meaning fewer symptoms of hyperactivity, impulsivity, and inattention, while higher scores indicate greater symptom severity. For the change scores used in the analysis, a negative value represents an improvement in symptoms (i.e., a decrease in the MOXO score from baseline), whereas a positive value indicates a worsening of symptoms (i.e., an increase in the MOXO score from baseline).
MOXO is the name of a continuous performance test (MOXO-CPT), a computerized assessment tool designed to aid in the diagnosis of ADHD by measuring attention, hyperactivity, impulsivity, and timing, incorporating visual and auditory distractors to simulate real-life environments. It is known for its high sensitivity (90%) and specificity (85%) in diagnosing ADHD41. It is an 18.2-minute test consisting of eight blocks, each containing 53 trials. During each trial, a stimulus (target or non-target) is presented in the center of the computer screen, followed by a “void” period of the same duration without stimuli. Participants are instructed to press the spacebar in response to targets and refrain from pressing it when non-targets are presented, all while ignoring a series of visual and auditory distractors. The blocks vary in cognitive load: two blocks are distractor-free, two include visual distractors, two have auditory distractors, and two combine both visual and auditory distractors. The following four performance indices are scored: (a) Attention: Number of correct responses performed within a predefined response time frame. (b) Timeliness: The number of correct answers performed only when the target stimulus was on the screen. (c) Hyperactivity: Number of commission responses that were not coded as impulsive responses. (d) Impulsivity: Number of commission responses performed when a non-target stimulus was present on the screen41. Changes (delta) in performance indices were calculated by subtracting the scores after the intervention from those obtained at baseline.
Additionally, the participants completed a short MATAL questionnaire at both time points. MATAL is the name of a standardized battery of tests used to assess learning disabilities in Hebrew-speaking populations. It is commonly used in Israel for educational and psychological evaluations. The MATAL questionnaire evaluates symptom severity using the ADHD Rating Scale-IV (ADHD RS). The short MATAL questionnaire consists of 89 statements assessing achievement and abilities in six domains: reading, writing, math, attention, visual perception and verbal memory42.
Long-term cortisol levels
We used FCC to assess the long-term, cumulative activity of the HPA axis in college students with ADHD. HCC has proven to validly capture the accumulated, integrated long-term activity of the HPA axis43,44,45. At baseline and after the intervention, participants were asked to cut the grown part of the nails from their ten fingers and place them into a sealable plastic bag. Samples were stored at room temperature until analysis. Cortisol was extracted as described by Warnock et al.46. In brief, the nails were washed twice with isopropanol and left to air-dry overnight. The dried nails were then transferred to a test tube with 5 mm zirconia balls and crushed in a mixer mill for 40 min, at 30 Hz. After milling, 15 mg of the resulting nail powder were incubated for 24 h in 1.5 ml methanol. The tube was then centrifuged, and 1 ml supernatant was transferred to a clean Eppendorf tube. The sample was thoroughly dried under nitrogen flow. Cortisol concentrations were determined using a commercial ELISA kit (EIA-CORT, RayBiotech, GA, USA), according to the manufacturer’s instructions.
Statistical analysis
Descriptive statistics were used to summarize independent variables for the two groups. T-tests were applied to assess the effectiveness of randomization. Since variables were not normally distributed, non-parametric independent T-tests (Mann–Whitney U test) and paired T-tests (Wilcoxon signed rank test) were used to examine differences between the groups. Categorical data were analyzed using the Chi-squared test. Spearman correlation coefficients were calculated to evaluate the relationships between MOXO test results and other quantitative variables. All statistical analyses were performed using SPSS software, version 23. Graphs were generated using GraphPad Prism 10.1.2 (GraphPad Software, Boston, Massachusetts USA, www.graphpad.com) and R studio version 4.3.2 (www.r-studio.com). p < 0.05 was considered significant.
To identify patterns of characteristics associated with greater benefits from the intervention, a multivariate analysis was conducted using a composite benefit score. This composite score was calculated based on improvements in academic grades, reductions in cortisol levels, and positive changes in behavioral outcomes, including attention, timing, hyperactivity, and impulsivity. Multiple regression analysis was performed to determine the relationship between participant characteristics (e.g., treatment group, age, gender, baseline scores) and the composite benefit score. The regression model was fitted using SPSS software, version 23 (SPSS Inc., Chicago, USA), and results were considered significant at p < 0.05.
Results
Demographics and baseline characteristics of the study group
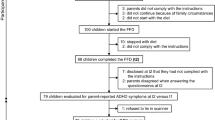
In total, 72 students responded to the emails calling for volunteers for the study. Five (6.9%) were excluded due to lack of interest (n = 3) or other reasons (n = 2), while 67 (93%) were enrolled and blindly randomized to receive either the probiotic or placebo treatment (33 and 34 students, respectively). Three participants from the placebo group were lost to follow-up and were excluded from the analysis. Additionally, three individuals randomly assigned to the probiotic group and one from the placebo group were removed due to the initiation of pharmacotherapy, which was in violation of an exclusion criteria. In total, 60 students completed the trial, 30 in each arm (Fig. 1). The raw data of the study are presented in Supplementary data S1.

Patient disposition flow diagram.
Table 1 summarizes the baseline demographics of the participants in the placebo and the probiotic groups. No statistically significant differences in demographic attributes were noted between the groups. Similarly, anthropometric measurements of average weight, BMI, fat percentage and waist circumference were not significantly different across groups at baseline or after a three-month intervention.
ADHD symptoms after intervention
ADHD attention, timeliness, hyperactivity and impulsivity were measured using the computerized MOXO performance test. A significant decrease in hyperactivity was documented after three months of the probiotic intervention (p = 0.012), while no changes in attention, timing, or impulsivity were noted (p > 0.05) (Fig. 2). In the placebo group, a significant reduction in impulsivity was measured after the intervention (p = 0.0036), while there were no significant changes in attention, timing, or hyperactivity (p > 0.05).

Attention deficit hyperactivity disorder (ADHD) symptoms before and after probiotics intervention: Levels of attention, timing, hyperactivity and impulsivity as measured using the MOXO performance test, in subjects receiving probiotic (blue columns; n = 30) or placebo (orange columns; n = 30) for three months. Light colors represent baseline scores, and dark colors represent post-intervention scores. BL = Baseline. Results are presented as mean ± SE. *p < 0.05, **p < 0.01 (Wilcoxon signed-rank test).
We divided participants into ‘normal-functioning’ and ‘low-functioning’ subgroups to explore whether baseline severity of symptoms moderated the treatment response. This division was based on the baseline MOXO performance indices, with the ‘low-functioning’ group including participants who had lower baseline scores across the majority of indices. This stratification allowed us to assess whether the probiotic intervention had differential effects depending on initial symptom severity. Participants in the ‘normal-functioning’ group had a baseline score higher than − 1 in all four tested performance indices, where more positive scores represent better outcomes. Participants with a baseline score of -1 or lower in at least one of the MOXO indices were included in the “low-functioning” group. Among the “low-functioning” subjects, those who consumed probiotics showed a significant improvement in hyperactivity (p = 0.0074), while no significant changes in attention, timing, or impulsivity were shown. For those receiving placebo, no changes were noted for MOXO scores (Fig. 3). Among the “high-functioning” subjects, no significant differences in MOXO scores were observed (p > 0.05) (data not shown).

Attention deficit hyperactivity disorder (ADHD) symptoms in the “low-functioning” subgroup: MOXO scores of attention, timing, hyperactivity and impulsivity in the low-functioning subjects treated with probiotics (blue columns; n = 24) or placebo (orange columns; n = 21) for three months. Light colors represent baseline scores, and dark colors represent post-intervention scores. BL = Baseline. Results are presented as mean ± SE. **p < 0.01 (Wilcoxon signed-rank test).
After three months of intervention no differences in the levels of MATAL-assessed attention and hyperactivity were noted in either group (p > 0.05), neither when considering all participants, nor when considering the “low functioning” subgroup only (data not shown).
Academic achievement
The academic achievement of each participant was calculated by comparing the average grades before entering the study to the grades after three months of intervention. Calculations were based on 17 students from the placebo group and 26 from the probiotic group since some did not provide their grade records. After three months of intervention, average grades were significantly increased in the probiotic group, whereas the improvement in the placebo group was only a nonsignificant trend (Table 2). We conducted a statistical analysis to compare the differences in average grades between the placebo and probiotic groups. The results showed a p-value of 0.4181 and an effect size (Cohen’s d) of -0.307, indicating that the difference between the two groups was not statistically significant.
Dietary intake and quality-of-life aspects
The FFQ questionnaire was used to profile nutritional intake at the study’s baseline (T0) and after three months of treatment. No significant differences in consumption of calories, proteins, carbohydrates, total sugars, fibers, fat, dairy products or total amount of vegetables and fruits were documented between groups. Notably, there was a significant increase in the consumption of total snacks and cakes in both groups after the three-month intervention (p < 0.01), with no differences between the two groups (Supplementary data S1).
While baseline GI symptoms score was similar in both groups (p = 0.884), a significant reduction (p-value = 0.007) in GI symptoms was reported in the probiotic group after three months of intervention, while no significant changes were reported in the placebo group (p > 0.05).
At baseline, the SSHS sleep pattern questionnaire found no significant differences in the total number of hours of sleep between the study groups (p = 0.97). After three months of intervention, no significant changes were noted in the total number of hours of sleep compared to baseline (p = 0.62) and between the two groups (p = 0.44). Similarly, according to the FEAHQ-36 questionnaire, no significant changes from baseline were measured in activity level, exposure to eating-promoting stimuli, responsiveness to hunger and satiety cues or eating style. These were not statistically different in either group (Supplementary data S1).
Correlations between ADHD performance indices, cortisol levels and academic outcomes
Baseline fingernail cortisol concentrations (FCC) were similar between the two groups (p-value = 0.614). No significant changes in long-term cortisol levels were observed in either group after the three-month intervention compared to the baseline, with no significant differences in the measured change between the two groups (Supplementary data S1).
Correlations between ADHD symptoms, as assessed by the MOXO test, average academic grades, and long-term cortisol levels were also explored (Fig. 4). Among “low-functioning” participants, a significant negative correlation between cortisol levels after the three-month intervention and attention and impulsivity was noted for those who received probiotics (rs=-0.478, p = 0.038, and rs = -0.731, p < 0.001, respectively). Furthermore, a significant negative correlation was identified in the probiotics group between cortisol levels after the three-month study period and the changes in timing (rs=-0.468, p-value = 0.043). In the probiotics group, there was also a significant positive correlation between the average final grades after the three-month intervention and changes in hyperactivity and impulsivity (rs = 0.554, p-value = 0.005 and rs = 0.520, p-value = 0.009, respectively) (Fig. 4).

Correlations between attention deficit hyperactivity disorder (ADHD) symptoms and academic grades and cortisol levels: Correlations between MOXO test results and fingernail cortisol levels (n = 19) and correlations between MOXO test results and academic grades (n = 24) in subjects receiving probiotics for three months. Colored dots display significant Spearman correlations - blue for negative relationships and red for positive. The intensity of the color corresponds to the strength of correlation as quantified by the correlation coefficient indicated inside each dot.
Multivariate analysis
To better understand the factors associated with greater benefit from the probiotic intervention, we conducted a multivariate analysis using a composite benefit score. This score was derived from improvements in academic grades, reductions in cortisol levels, and positive changes in behavioral outcomes, including attention, timing, hyperactivity, and impulsivity. Table 3 presents the results of the multiple regression analysis predicting the composite benefit score. The coefficients represent the estimated effect of each predictor variable on the composite benefit score, controlling for other variables in the model. Standard errors provide a measure of the variability of the coefficient estimates, while the t-statistics and p-values indicate the statistical significance of each predictor.
The model explains approximately 28.5% of the variance in the composite benefit score, indicating that the predictors have some explanatory power for the variation in benefits from the intervention. The analysis revealed that age was significantly associated with the composite benefit score (p = 0.013), with younger participants experiencing more substantial benefits from the intervention. Additionally, baseline cortisol levels were positively associated with the composite benefit score, though this finding was marginally significant (p = 0.095). This suggests that participants with higher initial cortisol levels might derive greater benefits from the probiotic treatment. Those in the treatment group, males, baseline weight and baseline academic grades were not significantly associated with the composite benefit score.
These findings highlight the importance of considering age when assessing the effectiveness of probiotic interventions in young adults with ADHD. The role of baseline cortisol levels warrants further investigation, as it may influence the extent to which individuals benefit from such treatments.
Standard errors (Std. Error) provide a measure of the variability of the coefficient estimates, while the t-statistics and p-values indicate the statistical significance of each predictor. p < 0.05 are shown in bold.
Discussion
This RCT examined the effects of a multi-strain probiotic supplement on ADHD symptoms, academic achievements, FCC, GI symptoms and sleep quality in college students with ADHD. The evaluations showed promising improvements in hyperactivity and academic performance among subjects who received probiotics compared to those who received placebo for three months. Moreover, improvements in ADHD symptoms correlated to lower cortisol levels.
Notably, the probiotic supplement reduced hyperactivity, as measured by the MOXO computational performance test, with a more pronounced benefit documented among participants with low baseline functioning. These results complement early-stage research, together suggesting that probiotics may exert beneficial effects across different ADHD symptom domains and populations47. However, it is important to note that these findings are preliminary, derived from limited studies, and require confirmation through more rigorous randomized controlled trials. The current study extended these findings to college students, suggesting that multi-strain probiotics may reduce hyperactivity in young adults with ADHD. Nevertheless, in this study, improvements were observed in hyperactivity but not in inattention or impulsivity.
The differential effects observed, where hyperactivity improved, but inattention and impulsivity did not, could be attributed to several factors. One possibility is that the specific strains of bacteria used in our study may have a more pronounced effect on hyperactivity-related pathways, such as those involved in motor activity and arousal, but may be less effective in modulating cognitive domains like attention and self-control. Previous studies that reported improvements in attention and self-control used different strains, or combinations of strains, which might have targeted neurotransmitter systems differently, such as those involved in executive function and cognitive control48.
It is also worth considering the role of the assessment tools used. The MOXO test, while effective in measuring various dimensions of ADHD symptoms, might be more sensitive to changes in hyperactivity compared to inattention or impulsivity. Differences in test sensitivity could explain why we observed significant improvements in one domain but not the others. Future studies could employ a broader range of assessment tools, including those specifically validated for measuring changes in attention and impulsivity, to capture a more comprehensive picture of the probiotic’s effects49 .
Another factor could be the interaction between the probiotics and the host’s unique microbiome composition, which could lead to variability in treatment response. Some bacterial strains might interact with the gut-brain axis in ways that preferentially influence hyperactivity, while other strains might be more effective in modulating cognitive processes underlying attention and self-control. This hypothesis suggests that personalized probiotic interventions, tailored to an individual’s microbiome composition, could potentially yield more consistent improvements across all ADHD symptom domains50,51.
Lower levels of academic achievement have been previously shown in college students with ADHD compared to their non-ADHD counterparts52, leading to increased dropout and lower occupational status53. Further, college students with ADHD are more likely to experience depression and anxiety54, which may delay their academic achievement. In the current work, significant improvements in academic grades were achieved by the end of the intervention among students taking probiotics compared to both their baseline performance and the placebo group. Moreover, higher academic grades were associated with lower MOXO scores in the hyperactivity and impulsivity domains, indicating that better academic performance correlated with reduced symptoms in these areas. In the MOXO test, lower scores represent better performance, with fewer symptoms of hyperactivity and impulsivity55.
Concerning the quality-of-life aspects examined in this study, probiotic supplementation did not affect sleep duration or eating habits. In contrast, GI symptoms improved after the probiotic intervention, which corroborates several studies, primarily in children, that highlighted the effectiveness of probiotic interventions in decreasing GI symptoms such as constipation, diarrhea, abdominal pain and flatulence56,57,58,59. Several GI morbidities are prevalent in adults with ADHD. A recent report found an increased rate of comorbid functional GI disorders (FGID), such as irritable bowel syndrome (IBS), in a large cohort of adults with ADHD60. These findings highlight the complex interplay between ADHD and GI function, where both may influence each other through shared pathways, such as autonomic dysfunction or immune dysregulation. The bidirectional communication of the gut-brain axis could play a role in this relationship, potentially contributing to the modulation of both GI symptoms and ADHD50,61, although further research is needed to fully understand these mechanisms.
In our study, we explored the relationship between attention, impulsivity, timeliness changes, and post-intervention cortisol levels within the low-function probiotics group, finding a significant negative correlation, especially with impulsivity. Fingernail cortisol, unlike blood or salivary cortisol, is unaffected by state-like confounders and may serve as a primary indicator of HPA axis activity62. Its role is crucial, given its widespread effects across the peripheral and central nervous system, influencing metabolism and cognition, factors pertinent to the development and persistence of stress-related disorders63. Our observations align with previous research indicating that subjects displaying diminished salivary cortisol levels post-stress are prone to committing more errors on attention tests, further underscoring the link between a blunted HPA axis response to stress and impulsivity observed in ADHD patients9.
However, no significant changes in cortisol levels were noted after the three-month intervention. A similar pilot study examining the effect of one week of B. longum supplementation on stress, anxiety and depression levels in 40 students, showed no substantial differences in these parameters between the probiotic vs. placebo groups64. In contrast, a one-month multi-strain probiotics treatment of 74 healthy undergraduate students preparing for an exam, improved psychological symptoms and lowered cortisol levels65. Further research will be needed to explain these conflicting reports.
While the study explored a range of primary and secondary outcomes, we recognize that multiple testing can increase the risk of Type I errors. To mitigate this risk, we conducted a multivariable analysis that accounted for multiple factors simultaneously, focusing on a composite benefit score derived from improvements in academic grades, reductions in cortisol levels, and behavioral outcomes. This approach allowed us to identify the most robust predictors of benefit from the intervention, providing a more reliable interpretation of the data. Nonetheless, we acknowledge that the potential for Type I errors remains, particularly in the analysis of secondary outcomes, and suggest that future studies with larger sample sizes and replication of findings are necessary to validate these results.
This study has several limitations. The single-center RCT had a modest sample size of 60 college students, with a mean age of 26, limits the generalizability of our findings to the broader adult ADHD population, particularly given the skewed gender distribution, with two-thirds being female. Additionally, while our results suggest potential benefits of probiotic treatment for ADHD symptoms, establishing a direct causal link remains challenging. Recent research emphasizes the importance of distinguishing between findings in pediatric and adult ADHD populations, highlighting the need for caution when extrapolating results from children to adults. Incorporating clinician-rated symptom scales alongside performance-based assessments, such as the MOXO test, could have strengthened conclusions regarding behavioral changes. Furthermore, 12 participants were withdrawn from the study due to non-adherence, with 5 participants starting drug treatment and 7 failing to consume at least 80% of the supplements. While full assessments were conducted for 4 out of the 5 participants who began drug treatment, these data were not carried forward in the final analysis due to the early termination and change in treatment conditions. This represents a limitation of the study, as it precludes an analysis of whether lower levels of adherence (e.g., 75% or 50%) might still yield beneficial outcomes. Future studies should explore the relationship between adherence levels and treatment efficacy to inform more flexible and inclusive study designs. Furthermore, while the study was conducted as a double-blind RCT, with the subjects, researchers, and statistician all blinded to the treatment allocations, no formal check of blinding (such as asking participants to guess their treatment assignment) was performed. This represents a limitation of the study, as it precludes an evaluation of the effectiveness of the blinding process, which could potentially impact the interpretation of the results. Future studies should consider including such a check to ensure the robustness of the blinding process. Finally, measuring inflammatory biomarkers and gut microbiome profiles before and after treatment could have helped elucidate biological mechanisms underlying the beneficial effects of probiotics.
In summary, this double-blind RCT was the first to show significant improvements in ADHD symptoms among college students receiving probiotic supplementation. This study suggests probiotics as a potential treatment approach to ease ADHD symptoms in this population. The presented findings set the stage for larger multi-center trials designed to examine multi-strain probiotic formulas to enhance functional outcomes in individuals with ADHD. Identifying the specific bacterial strains, dosages and population sub-groups that stand to most benefit from such treatment will help optimize and advance this promising microbiome-directed strategy.
Data availability
Data availability: All data generated or analyzed during this study are included in this published article Supplementary data S1.
References
DuPaul, G. J., Pollack, B. & Pinho, T. D. Attention-deficit/hyperactivity disorder. In Handbook of DSM-5 disorders in children and adolescents (eds Goldstein, S. & DeVries, M.) 399–416 (Springer, Cham, 2017).
Ayano, G. et al. Prevalence of attention deficit hyperactivity disorder in adults: Umbrella review of evidence generated across the globe. Psychiatry Res.328, 115449. https://doi.org/10.1016/j.psychres.2023.115449 (2023).
Song, P. et al. The prevalence of adult attention-deficit hyperactivity disorder: A global systematic review and meta-analysis. J Glob Health11, 04009. https://doi.org/10.7189/jogh.11.04009 (2021).
Custodio, R. J. P. et al. Adult ADHD: It is old and new at the same time – what is it?. Rev. Neurosci.35, 225–241. https://doi.org/10.1515/revneuro-2023-0071 (2024).
Weyandt, L. L. & Dupaul, G. J. ADHD in college students: Developmental findings. Dev Disabil Res Rev14, 311–319. https://doi.org/10.1002/ddrr.38 (2008).
Kessler, R. C. et al. The prevalence and correlates of adult ADHD in the United States: Results from the national comorbidity survey replication. Am J Psychiat.163, 716–723. https://doi.org/10.1176/ajp.2006.163.4.716 (2006).
Bauer, A. M., Quas, J. A. & Boyce, W. T. Associations between physiological reactivity and children’s behavior: Advantages of a multisystem approach. J. Develop. Behav. Pediatr.23, 102–113. https://doi.org/10.1097/00004703-200204000-00007 (2002).
Griffiths, K. R. et al. Sustained attention and heart rate variability in children and adolescents with ADHD. Biol. Psychol.124, 11–20. https://doi.org/10.1016/j.biopsycho.2017.01.004 (2017).
Hong, H. J., Shin, D. W., Lee, E. H., Oh, Y. H. & Noh, K. S. Hypothalamic-pituitary-adrenal reactivity in boys with attention deficit hyperactivity disorder. Yonsei Med. J.44, 608. https://doi.org/10.3349/ymj.2003.44.4.608 (2003).
Blomqvist, M. et al. Salivary cortisol levels and dental anxiety in children with attention deficit hyperactivity disorder. Eur. J. Oral Sci.115, 1–6. https://doi.org/10.1111/j.1600-0722.2007.00423.x (2007).
Kamradt, J. M., Momany, A. M. & Nikolas, M. A. A meta-analytic review of the association between cortisol reactivity in response to a stressor and attention-deficit hyperactivity disorder. ADHD Atten Def Hyp Disord10, 99–111. https://doi.org/10.1007/s12402-017-0238-5 (2018).
Takada, M. et al. Probiotic Lactobacillus casei strain shirota relieves stress-associated symptoms by modulating the gut-brain interaction in human and animal models. Neurogastroenterol Motil28, 1027–1036. https://doi.org/10.1111/nmo.12804 (2016).
Kato-Kataoka, A. et al. Fermented milk containing lactobacillus casei strain shirota preserves the diversity of the gut microbiota and relieves abdominal dysfunction in healthy medical students exposed to academic stress. Appl Environ Microbiol82, 3649–3658. https://doi.org/10.1128/AEM.04134-15 (2016).
Langkamp-Henken, B. et al. Bifidobacterium Bifidum R0071 results in a greater proportion of healthy days and a lower percentage of academically stressed students reporting a day of cold/Flu: A randomised, double-blind Placebo-Controlled Study. Br. J. Nutr.113, 426–434. https://doi.org/10.1017/S0007114514003997 (2015).
Rogers, G. B. et al. From gut dysbiosis to altered brain function and mental illness: Mechanisms and pathways. Mol Psychiatry21, 738–748. https://doi.org/10.1038/mp.2016.50 (2016).
Checa-Ros, A., Jeréz-Calero, A., Molina-Carballo, A., Campoy, C. & Muñoz-Hoyos, A. Current evidence on the role of the gut microbiome in ADHD pathophysiology and therapeutic implications. Nutrients13, 249. https://doi.org/10.3390/nu13010249 (2021).
Dinan, T. G., Stanton, C. & Cryan, J. F. Psychobiotics: A novel class of psychotropic. Biol. Psychiatry74, 720–726. https://doi.org/10.1016/j.biopsych.2013.05.001 (2013).
Fang, Z. et al. Bifidobacterium longum mediated tryptophan metabolism to improve atopic dermatitis via the gut-skin axis. Gut Microbes14, 2044723. https://doi.org/10.1080/19490976.2022.2044723 (2022).
Hara, T., Mihara, T., Ishibashi, M., Kumagai, T. & Joh, T. Heat-Killed Lactobacillus Casei Subsp. Casei 327 Promotes colonic serotonin synthesis in mice. J. Funct. Food47, 585–589. https://doi.org/10.1016/j.jff.2018.05.050 (2018).
Nimgampalle, M. & Kuna, Y. Anti-alzheimer properties of probiotic, lactobacillus plantarum MTCC 1325 in alzheimer’s disease induced albino rats. J. Clin. Diagn. Res.11, KC 01-KC05. https://doi.org/10.7860/JCDR/2017/26106.10428 (2017).
Vasiliu, O. The current state of research for psychobiotics use in the management of psychiatric disorders–A systematic literature review. Front Psychiathttps://doi.org/10.3389/fpsyt.2023.1074736 (2023).
Sakurai, T., Odamaki, T. & Xiao, J. Production of Indole-3-Lactic acid by bifidobacterium strains isolated from human infants. Microorganisms7, 340. https://doi.org/10.3390/microorganisms7090340 (2019).
Bjerre, K. et al. Development of bacillus subtilis mutants to produce tryptophan in pigs. Biotechnol Lett39, 289–295. https://doi.org/10.1007/s10529-016-2245-6 (2017).
Hussain, S., Andrews, D. & Hill, B. C. Using tryptophan mutants to probe the structural and functional status of BsSCO, a copper binding, cytochrome c oxidase assembly protein from bacillus subtilis. Biochemistry56, 6355–6367. https://doi.org/10.1021/acs.biochem.7b00833 (2017).
Cheng, H. W., Jiang, S., Hu, J., Cheng, H. W., Jiang, S., & Hu, J. Gut-brain axis: Probiotic, <em>Bacillus Subtilis</Em>, Prevents aggression via the modification of the central serotonergic system. in oral health by using probiotic products; IntechOpen, 2019 ISBN 978-1-83968-140-0.
Wang, W. C., Yan, F. F., Hu, J. Y., Amen, O. A. & Cheng, H. W. Supplementation of bacillus subtilis-based probiotic reduces heat stress-related behaviors and inflammatory response in broiler chickens. J Anim Sci96, 1654–1666. https://doi.org/10.1093/jas/sky092 (2018).
Zaghari, M., Zahroojian, N., Riahi, M. & Parhizkar, S. Effect of bacillus subtilis spore (GalliPro®) nutrients equivalency value on broiler chicken performance. J. Animal Sci. Italhttps://doi.org/10.4081/ijas.2015.3555 (2015).
Takahashi, K. et al. Effect of enterococcus faecalis 2001 on colitis and depressive-like behavior in dextran sulfate sodium-treated mice: Involvement of the brain-gut axis. J. Neuroinflamm.16, 201. https://doi.org/10.1186/s12974-019-1580-7 (2019).
Reis, D. J., Ilardi, S. S. & Punt, S. E. W. The anxiolytic effect of probiotics: A systematic review and meta-analysis of the clinical and preclinical literature. PLOS ONE13, e0199041. https://doi.org/10.1371/journal.pone.0199041 (2018).
Pärtty, A., Kalliomäki, M., Wacklin, P., Salminen, S. & Isolauri, E. A possible link between early probiotic intervention and the risk of neuropsychiatric disorders later in childhood: A randomized trial. Pediatr Res77, 823–828. https://doi.org/10.1038/pr.2015.51 (2015).
Wang, L.-J. et al. Effect of bifidobacterium bifidum on clinical characteristics and gut microbiota in attention-deficit/hyperactivity disorder. J Pers Med12, 227. https://doi.org/10.3390/jpm12020227 (2022).
Messaoudi, M. et al. Assessment of psychotropic-like properties of a probiotic formulation (lactobacillus helveticus R0052 and bifidobacterium longum R0175) in rats and human subjects. Br. J. Nutr.105, 755–764. https://doi.org/10.1017/S0007114510004319 (2011).
Wang, Z. et al. Absence of causal relationship between levels of unsaturated fatty acids and ADHD: evidence from mendelian randomization study. J. Atten. Disord.https://doi.org/10.1177/10870547241264660 (2024).
Abramson, J. H. WINPEPI updated: Computer programs for epidemiologists, and their teaching potential. Epidemiol Perspect Innov8, 1. https://doi.org/10.1186/1742-5573-8-1 (2011).
Akkasheh, G. et al. Clinical and metabolic response to probiotic administration in patients with major depressive disorder: A randomized, double-blind placebo-controlled trial. Nutrition32, 315–320. https://doi.org/10.1016/j.nut.2015.09.003 (2016).
Shahar, D., Fraser, D., Shai, I. & Vardi, H. Development of a food frequency questionnaire (FFQ) for an elderly population based on a population survey. J Nutr133, 3625–3629. https://doi.org/10.1093/jn/133.11.3625 (2003).
Moshfegh, A. J. et al. The US department of agriculture automated multiple-pass method reduces bias in the collection of energy intakes. Am. J. Clin. Nutrit.88, 324–332. https://doi.org/10.1093/ajcn/88.2.324 (2008).
Golan, M. & Weizman, A. Reliability and validity of the family eating and activity habits questionnaire. Eur. J. Clin. Nutr.52, 771–777. https://doi.org/10.1038/sj.ejcn.1600647 (1998).
Wolfson, A. R. et al. Evidence for the validity of a sleep habits survey for adolescents. Sleep26, 213–216. https://doi.org/10.1093/sleep/26.2.213 (2003).
Bytzer, P. et al. Prevalence of gastrointestinal symptoms associated with diabetes mellitus: A population-based survey of 15,000 adults. Arch. Intern. Med.161, 1989–1996. https://doi.org/10.1001/archinte.161.16.1989 (2001).
Berger, I. & Goldzweig, G. Objective measures of attention-deficit/hyperactivity disorder: A pilot study. Isr. Med. Assoc. J.12, 531–535 (2010).
Ben-Simon, A. & Inbar-Weiss, N. MATAL test battery for the diagnosis of learning disabilities: User Guide. (2012).
Izawa, S. et al. Cortisol level measurements in fingernails as a retrospective index of hormone production. Psychoneuroendocrinology54, 24–30. https://doi.org/10.1016/j.psyneuen.2015.01.015 (2015).
Izawa, S., Sugaya, N., Ogawa, N., Shirotsuki, K. & Nomura, S. A validation study on fingernail cortisol: Correlations with one-month cortisol levels estimated by hair and saliva samples. Stress24, 734–741. https://doi.org/10.1080/10253890.2021.1895113 (2021).
Herane-Vives, A. et al. Elevated fingernail cortisol levels in major depressive episodes. Psychoneuroendocrinology88, 17–23. https://doi.org/10.1016/j.psyneuen.2017.10.026 (2018).
Warnock, F. et al. Measuring cortisol and DHEA in fingernails: A pilot study. Neuropsychiatr Dis Treat6, 1–7 (2010).
Wang, Y. et al. Probiotics and fructo-oligosaccharide intervention modulate the microbiota-gut brain axis to improve autism spectrum reducing also the hyper-serotonergic state and the dopamine metabolism disorder. Pharmacol Res157, 104784. https://doi.org/10.1016/j.phrs.2020.104784 (2020).
Slykerman, R. F. et al. Effect of lactobacillus rhamnosus HN001 in pregnancy on postpartum symptoms of depression and anxiety: A randomised double-blind placebo-controlled trial. EBioMedicine24, 159–165. https://doi.org/10.1016/j.ebiom.2017.09.013 (2017).
Tamm, L., Epstein, J. N., Peugh, J. L., Nakonezny, P. A. & Hughes, C. W. Preliminary data suggesting the efficacy of attention training for school-aged children with ADHD. Dev Cogn Neurosci4, 16–28. https://doi.org/10.1016/j.dcn.2012.11.004 (2013).
Borre, Y. E., Moloney, R. D., Clarke, G., Dinan, T. G. & Cryan, J. F. The impact of microbiota on brain and behavior: Mechanisms & therapeutic potential. Adv Exp Med Biol817, 373–403. https://doi.org/10.1007/978-1-4939-0897-4_17 (2014).
Voreades, N., Kozil, A. & Weir, T. L. Diet and the development of the human intestinal microbiome. Front Microbiol5, 494. https://doi.org/10.3389/fmicb.2014.00494 (2014).
Frazier, T. W., Youngstrom, E. A., Glutting, J. J. & Watkins, M. W. ADHD and achievement: Meta-analysis of the child, adolescent, and adult literatures and a concomitant study with college students. J Learn Disabil40, 49–65. https://doi.org/10.1177/00222194070400010401 (2007).
Kuriyan, A. B. et al. Young adult educational and vocational outcomes of children diagnosed with ADHD. J Abnorm Child Psychol41, 27–41. https://doi.org/10.1007/s10802-012-9658-z (2013).
Nelson, J. M. & Gregg, N. Depression and anxiety among transitioning adolescents and college students with ADHD, dyslexia, or comorbid ADHD/dyslexia. J Atten Disord16, 244–254. https://doi.org/10.1177/1087054710385783 (2012).
Skott, E. et al. Effects of a synbiotic on symptoms, and daily functioning in attention deficit hyperactivity disorder - A double-blind randomized controlled trial. Brain Behav Immun89, 9–19. https://doi.org/10.1016/j.bbi.2020.05.056 (2020).
Almog, M., Gabis, L. V., Shefer, S. & Bujanover, Y. Gastrointestinal symptoms in pediatric patients with attention deficit and hyperactivity disorders. Harefuah149(33–36), 62 (2010).
Jameson, N. D. et al. Medical comorbidity of attention-deficit/hyperactivity disorder in US adolescents. J Child Neurol31, 1282–1289. https://doi.org/10.1177/0883073816653782 (2016).
McKeown, C., Hisle-Gorman, E., Eide, M., Gorman, G. H. & Nylund, C. M. Association of constipation and fecal incontinence with attention-deficit/hyperactivity disorder. Pediatrics132, e1210–e1215. https://doi.org/10.1542/peds.2013-1580 (2013).
Ming, X. et al. A gut feeling: A hypothesis of the role of the microbiome in attention-deficit/hyperactivity disorders. Child Neurology Openhttps://doi.org/10.1177/2329048X18786799 (2018).
Kedem, S. et al. Attention deficit hyperactivity disorder and gastrointestinal morbidity in a large cohort of young adults. World J Gastroenterol26, 6626–6637. https://doi.org/10.3748/wjg.v26.i42.6626 (2020).
Cryan, J. F. & Dinan, T. G. Mind-altering microorganisms: The impact of the gut microbiota on brain and behaviour. Nat Rev Neurosci13, 701–712. https://doi.org/10.1038/nrn3346 (2012).
Fischer, S., Schumacher, S., Skoluda, N. & Strahler, J. Fingernail cortisol – state of research and future directions. Front. Neuroendocrinol.58, 100855. https://doi.org/10.1016/j.yfrne.2020.100855 (2020).
Knezevic, E., Nenic, K., Milanovic, V. & Knezevic, N. N. The role of cortisol in chronic stress, neurodegenerative diseases, and psychological disorders. Cells12, 2726. https://doi.org/10.3390/cells12232726 (2023).
Siegel, M. P. & Conklin, S. M. Acute intake of B. Longum probiotic does not reduce stress, anxiety, or depression in young adults: A pilot study. Brain Behav Immun Health2, 100029. https://doi.org/10.1016/j.bbih.2019.100029 (2020).
Venkataraman, R. et al. Effect of multi-strain probiotic formulation on students facing examination stress: A double-blind, Placebo-controlled study. Probiotics Antimicrob Proteins13, 12–18. https://doi.org/10.1007/s12602-020-09681-4 (2021).
Acknowledgements
The authors wish to thank the Tel Hai Academic College Support Center and Mrs. Tami Buzagloo for their professional assistance during the trial. We thank Dr. Nadya Lisovoder, Mrs. Inas Davor and Mrs. Ester Vinstov for support and advice regarding the study design.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
MS conducted the research, collected the data and performed the statistical analysis. FM performed the cortisol experiments and wrote the original draft of manuscript. IY helped with the statistical analysis. ST had primary responsibility for the conception, funding acquisition and design of the study. All authors contributed to the manuscript revision and read and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Levy Schwartz, M., Magzal, F., Yehuda, I. et al. Exploring the impact of probiotics on adult ADHD management through a double-blind RCT. Sci Rep 14, 26830 (2024). https://doi.org/10.1038/s41598-024-73874-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-73874-y
